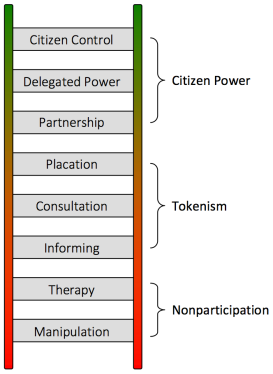
Arnstein’s ladder of citizen participation and inclusion. It represents the redistribution of power that enables marginalised citizens, presently excluded from the political and economic processes, to be purposefully included in the future.
The government’s Work and Health Programme, due to be rolled out this autumn, involves a plan to integrate health and employment services, aligning the outcome frameworks of health services, Improving Access to Psychological Therapies (IAPT), Jobcentre Plus and the Work Programme.
But the government’s aim to prompt public services and commissioned providers to “speak with one voice” is founded on traditional Conservative prejudices about people who need support. This proposed multi-agency approach is reductive, rather than being about formulating expansive, coherent, comprehensive and importantly, responsive mental health provision.
What’s on offer is psychopolitics, not therapy. It’s about (re)defining the experience and reality of a marginalised social group to justify dismantling public services (especially welfare). In linking receipt of welfare with health services and state therapy, with the single politically intended outcome of employment, the government is purposefully conflating citizens’ widely varied needs with economic outcomes and diktats, which will isolate people from traditionally non-partisan networks of unconditional support, such as the health service, social services, community services and mental health services.
Services “speaking with one voice” will invariably make accessing support conditional, and further isolate marginalised social groups. It will damage trust between people needing support and professionals who are meant to deliver essential public services, rather than simply extending government dogma, prejudices and discrimination. And meeting ideologically designed targets.
As neoliberals, the Conservatives see the state as a means to reshape social institutions and social relationships hierarchically, based on a model of a competitive market place. This requires a highly invasive power and mechanisms of persuasion, manifested in an authoritarian turn. Public interests are conflated with narrow economic outcomes. Public behaviours are politically micromanaged and modified. Social groups that don’t conform to ideologically defined economic outcomes and politically defined norms are stigmatised and outgrouped.
Othering and outgrouping have become common political practices, it seems.
The Work and Health Programme is a welfare-to-work programme for people with disabilities, mental health problems and for long-term unemployed people, due to be rolled out in the autumn. In the recent Work, Health and Disability green paper, the government mentioned new mandatory “health and work conversations” in which work coaches will use “specially designed techniques” to “help” those people in the ESA Support Group – those assessed by their own doctors and the state as being unlikely to work in the near future – “identify their health and work goals, draw out their strengths, make realistic plans, and build resilience and motivation.”
Apparently these “conversations” were “co-designed” by the Behavioural Insights Team.
Democracy is based on a process of dialogue between the public and government, ensuring that the public are represented: that governments are responsive, shaping policies that address identified social needs.
However, policies increasingly reflect a behaviourist turn. They are no longer about reflecting citizens’ needs: they are increasingly about telling some citizens how to be. This has some profound implications for democracy.
Neoliberal policies increasingly extend behaviour modification techniques that aim to quantifiably change the perceptions and behaviours of citizens, aligning them with narrow neoliberal outcomes through rewards or “consequences.” Rewards, such as tax cuts, are aimed at the wealthiest, whereas the most vulnerable citizens who are the poorest are simply presented with imposed cuts to their lifeline support as an “incentive” to not be poor. Taking money from the poorest is apparently “for their own good”.
Defining human agency and rationality in terms of economic outcomes is extremely problematic. And dehumanising. Despite the alleged value-neutrality of behavioural economic theory and CBT, both have become invariably biased towards the status quo rather than progressive change and social justice.
Behavoural economics theory has permited policy-makers to indulge ideological impulses whilst presenting them as “objective science.” From a libertarian paternalist perspective, the problems of neoliberalism don’t lie in the market, or in growing inequality and poverty: neoliberalism isn’t flawed, nor are governments – we are. Governments and behavioural economists don’t make mistakes – only citizens do. No-one is nudging the nudgers. It’s assumed that their decision-making is infallible and they have no whopping cognitive biases of their own.
“There’s no reason to think that markets always drive people to what’s good for them.” Richard Thaler.
There’s no reason whatsoever to think that markets are good for people at all. Let’s not confuse economics with psychology, or competitive individualism and economic Darwinism with collectivism and mutual aid. Behavioural economics may offer us titbit theories explaining individual consumer’s decision making, but it’s been rather unreliable in explaining socioeconomic and political contexts and complex systems such as financial crises, and of course behavioual economists don’t feel the same pressing need to explore the decision making and “cognitive bias” of the handful of people who cause those.
It wasn’t those with mental health problems currently claiming social security. They do much less damage to the economy, in fact IAPT means vulture capitalist private companies like G4S and trusts like Southern Care can turn a profit offering “support”.
The current emphasis on quantitative methodology and standardisation has led to an overwhelming focus on measurement in IAPT settings. Mental health services are now dominated by IAPT, which focuses exclusively on “evidence-based” and short-term interventions for clients with particular diagnoses – mostly anxiety disorders and depression. Most workers in IAPT services offer CBT, often by minimally trained psychological wellbeing practitioners offering “low-intensity” interventions over few sessions.
Verificationism and standardisation leads to a focus on measurement in IAPT settings. CBT mutes the causes of distress, which do not reside “within” the individual: they are intersubjectively constructed, with cultural, socioeconomic and political dimensions. Furthermore, there is little room left for authentic dialogue – qualitative accounts of client’s experiences are not accommodated. In this context, CBT is authoritarian, rather than being prefigurative and genuinely dialogic.
Under the government’s plans, therapists from the IAPT programme are to support jobcentre staff to assess and treat claimants, who may be referred to online cognitive behavioural therapy (CBT) courses.
We must question the ethics of linking receipt of welfare with “state therapy,” which, upon closer scrutiny, is not therapy at all. Linked to such a narrow outcome – getting a job – it amounts to little more than a blunt behaviour modification programme. The fact that the Conservatives have planned to make receipt of benefits contingent on participation in “treatment” also worryingly takes away the fundamental right of consent.
CBT facilitates the identification of “negative thinking patterns” and associated “problematic behaviours” and “challenges” them. This approach is at first glance a problem-solving approach, however, it’s of course premised on the assumption that interpreting situations “negatively” is a bad thing, and that thinking positively about bad events is beneficial.
The onus is on the individual to adapt by perceiving their circumstances in a stoical and purely “rational” way.
So we need to ask what are the circumstances that we expect people to accept stoically. Socioeconomic inequality? Precarity? Absolute poverty? Sanctions? Work fare? Being forced to accept very poorly paid work, abysmal working conditions and no security? The loss of social support, public services and essential safety nets? Starvation and destitution?
It’s all very well challenging people’s thoughts but for whom is CBT being used. For what purpose? It seems to me that this is about coercing those people on the wrong side of draconian government policy to accommodate that; to mute negative responses to negative situations. CBT in this context is not based on a genuinely liberational approach, nor is it based on democratic dialogue. It’s about modifying and controlling behaviour, particularly when it’s aimed at such narrow, politically defined and specific economic outcomes, which extend and perpetuate inequality. In this context, CBT becomes state “therapy” used only as an ideological prop for neoliberalism.
CBT tends to generate oversimplifications of the causes human distress. It’s not about helping people make better choices, it’s about coercing people to make the choices that policymakers want them to make. Those “choices” are based on enforced conformity to the ideological commitments of policymakers.
It’s assumed that the causes of unemployment are personal and attitudinal rather than sociopolitical or because of health barriers, and that particular assumption authorises intrusive state interventions that encode a Conservative moral framework, which places responsibility on the individual, who is characterised as “faulty” in some way. The deeply flawed political/economic system that entrenches inequality isn’t challenged at all: its victims are discredited and stigmatised instead.
Yet historically (and empirically), it has been widely accepted that poverty significantly increases the risk of mental health problems and can be both a causal factor and a consequence of mental ill health. Mental health is shaped by the wide-ranging characteristics and circumstances (including inequalities) of the social, economic and physical environments in which people live. Successfully supporting the mental health and wellbeing of people living in poverty, and reducing the number of people with mental health problems experiencing poverty, requires engagement with this complexity.
There is also widely held assumption that working is good for mental health, and that being in employment indicates mental wellbeing. It’s well-established that poverty is strongly linked with a higher likelihood of being diagnosed with a mental illness. That does not mean working is therefore somehow “good” for mental health. Encouraging people to work should entail genuine support, it shouldn’t entail taking away their lifeline income as punishment “incentive” if they can’t work.
An adequate level of social security to meet people’s basic survival needs is not mutually exclusive from encouraging people to find a suitable job.
It’s worth noting that research indicates in countries with an adequate social safety net, poor employment (low pay, short-term contracts), rather than “worklessness”, has the biggest detrimental impact on mental health.
CBT does not address the socioeconomic and political context. It permits society to look the other way, whilst the government continue to present mental illness as an individual weakness or vulnerability, and a consequence of “worklessness” rather than a fairly predictable result of living a distressing, stigmatised, excluded existence and material deprivation in an increasingly unequal society.
Inequality and poverty arise because of ideology and policy-formulated socioeconomic circumstances, but the government have transformed established explanations into a project of constructing behavioural and cognitive problems as “medical diagnoses” for politically created socioeconomic problems. Austerity targets the poorest disproportionately for cuts to income and essential services, it’s one ideologically-driven political decision taken amongst alternative, effective and more humane choices.
Both nudge and CBT are being used to prop up austerity and reflect neoliberal managementspeak at its very worst. Neoliberal policies are causing profound damage, harm and distress to those they were never actually designed to “help”. Let’s not permit techniques of neutralisation: the use of rhetoric to obscure the real intention behind policies. It’s nothing less than political gaslighting.
The government’s profound antiwelfarist rhetoric indicates that there’s no genuine intention to support those people with mental health problems and others in need, despite their semantic thrifts and diversions.
Policies are expressed political intentions regarding how our society is organised and governed. They have calculated social and economic aims and consequences. In democratic societies, all citizen’s accounts of the impacts of policies ought to matter.
However, in the UK, the way that policies are justified is being increasingly detached from their aims and consequences, partly because democratic processes and basic human rights are being disassembled or side-stepped, partly because the government employs the widespread use of linguistic strategies and techniques of persuasion to intentionally divert us from the aims and consequences of their ideologically driven and increasingly dehumanising policies. Furthermore, policies have become increasingly detached from public interests and needs.
For people with mental health problems, policies are being formulated to act upon them as if they are objects, rather than autonomous human subjects. Such a dehumanising approach has contributed significantly to a wider process of social outgrouping, increasing stigmatisation and ultimately, to further socioeconomic and mental health inequalities.
It’s the government that need to change their behaviour.
It’s us that need to make a stand against hegemonic neoliberal discourse and injustice.

—
This article was written for a zine to mark the protest at the 10th annual New Savoy conference on 15 March in London #newsavoy2017. You can read the zine, with other people’s excellent contributions, here.
Also, see: New Savoy Protest against psycho-compulsion of MH claimants – 15th March 2017.
You can read about the background to the Mental Wealth Alliance and the New Savoy demo and lobby here.
You can watch the video here from Let Me Look TV: Protest at the 10th Annual New Savoy Conference 15 March 2017.
Please share.
Related
The power of positive thinking is really political gaslighting
The importance of citizen’s qualitative accounts in democratic inclusion and political participation
A critique of the ‘Origins of Happiness’ study
A critique of Conservative notions of social research
Research finds damaging mental health discrimination ‘built into’ Work Capability Assessment. Again.
The Conservative approach to social research – that way madness lies
I don’t make any money from my work. I am disabled because of illness and have a very limited income. The budget didn’t do me any favours at all.
But you can help by making a donation to help me continue to research and write informative, insightful and independent articles, and to provide support to others. The smallest amount is much appreciated – thank you.

![]()


Reblogged this on sdbast.
LikeLike
I am dreading this. I have been told by NHS that they don’t have any suitable support for me and gave me a name of a charity to help me. They are now only bothered with me when I am in crisis and sectionable or in the morg. If the gov try to use this on me I will not survive and/ they won’t because if they put me in the position of killing myself I am quite willing to take one of them with me what have I got to lose? Totally freaked out. BPD/PTSD/Deppression/anxiety
LikeLike
Hi, I am sorry about your circumstances and how you feel. Firstly, I hope the charity can offer you some support, and hope you give that a try. You’re right that the service tends to wait until you are in crisis before they act – which is too late. It’s a firefighting approach and a lot of it is down to lack of funding and resources, but that doesn’t help you.
You can also try this – https://freepsychotherapynetwork.com/find-an-therapist/
Let us know how you get on, and if you need to talk, you can anytime here, and in private if you wish. Best wishes x
LikeLiked by 1 person
As I psychologist working in an IAPT service I don’t recognise your construction of CBT or of IAPT. Neither are value laden, CBT is a technology and IAPT is a system of delivery. They can be used for transformative and liberating purposes or they can be used produce conformity. If you have a “core belief” that everyone will reject you this is profoundly debilitating. If a therapy can provide a space to adjust this, the patient gets the chance to operate without that burden. Whether this allows them to achieve greater political solidarity or to get a job at distribution centre is really up to them.
I’ve no doubt that there are bad IAPT services and I strongly suspect these are predominantly delivered by private providers. However, you have to be careful in what you say bacause you risk alienating fellow travellers within the allied professions.
LikeLike
CBT is a “technology”? IAPT is a “system of delivery”? That’s a very mechanistic, positivistic and profoundly alienating language which doesn’t sit well with me, since we are discussing interactions with fellow human beings, not some objects to be “adjusted” so they can “operate”.
There is little else on offer via IAPT but CBT. Regardless of your view of CBT as a therapeutic model, the fact that it is being used to coerce people into getting a job, and that there are no alternative therapies on offer is worrying. At best, surely you can concede that CBT doesn’t suit everyone. But my point about it being used as a political tool to conflate people’s needs with their employment status is a real one, sadly.
I am sure that CBT may well be used to help some people, but those being offered it are not only people with self esteem issues, unfortunately. Many have very complex conditions that do not respond to CBT.
And CBT really doesn’t work for everyone. I was a trained social work practitioner.
As a “fellow traveller”, I would expect that you would recognise that my concern is about alienating those people we are supporting, not colleagues. Many colleagues recognise that we face a danger of being coopted by the government to deliver a limited and limiting type of remarkably partisan, value-laden therapy. It’s not possible to support people without acknowledging the profound impacts that their context has on them. It’s my view that it’s not possible to practice value-free therapy, nor is it sufficient. Without addressing the problems that our socioeconomic and political context imposes on all of us, we all become oppressed and potentially, oppressive, when we expect that others simply live with adverse material and subsequently untenable situations, distressing and limiting life experiences and psychological conditions.
Have a read of the Samaritans latest report. It links inequality and poverty with increasing suicide. I read it and it made me so angry. It SHOULD make people very angry. We’re one of the wealthiest nations on earth, yet people are living in absolute poverty. If people can’t meet their basic survival needs, there is little chance they will be able meet psychosocial ones.
Your point about private companies is a very good one, and given that many are driven by a profit motive and “efficiency”, that does have an impact on both the quality of training and subsequently, practitioner’s level of competence. The Southern Trust is a very good example of this, and the fact that G4S are recuiting CBT therapists to deliver in the NHS is another big cause for concern, given their long list of human rights abuses on a global scale.
LikeLiked by 5 people
A real psychologist in an IAPT service? I’m shocked. When IAPT was rolled out, the psychology budgets of the CMHTs in my area were sucked into it. As a result, people with more complex needs lost out.
Why? Because IAPT services are risk averse. CBT for all, as long as they’re not too unwell…
Which is probably a good thing for me as some poorly trained twit telling me that my life isn’t shit because it’s shit, but because I think it’s shit is really not going to help.
And now politicians, ably assisted by the likes of M***, are weaponising your “technology”.
As a psychologist, I’m sure you are aware that there is no effective outcomes framework in MH. Yet work is being sold as an outcome.
I am not “stock”, or a unit of productivity.
LikeLiked by 3 people
None of us are “stock” and being in paid employment to profit an employer is not the only way of being “productive.” It’s shameful to reduce human lives and experiences to prop up a neoliberal economy and ideology and regarding those who suffer as some kind of inevitable “collateral damage”. Even worse, denying that it’s an inevitable feature of the socioeconomic and political context by blaming the individual is unforgivable. It’s gaslighting.
LikeLiked by 3 people
Reblogged this on Alliance blog and commented:
“For people with mental health problems, policies are being formulated to act upon them as if they are objects, rather than autonomous human subjects.”
Essential reading…
LikeLiked by 2 people
Reblogged this on Declaration Of Opinion and commented:
Recovery in a time limit. “Therapy” six-sessions then off you go on your own again. These politicians are such backwards thinkers still hammering the “work work work” message into people. All forward thinking democracies are looking at the near future where work is going to be in very limited supply because of technology, rising populations mean more people, less work, these people will need supporting unless population control or culling is on the agenda? And the way this Govt has been behaving that’s not out of the bounds of possibility.
LikeLiked by 1 person
Reblogged this on perfectlyfadeddelusions.
LikeLiked by 1 person
The evil Neoliberal Conservative politicians are psychopaths who are physically unable to experience any human compassion or empathy, are utterly charming, lie frequently, take risks and like psychopaths always blame others for their problems, their incompetence and only care about themselves.
If psychopaths were banned from political office then politics and social policy would become far more humane and adopt people first policies.
LikeLiked by 1 person
I’m a Social Work student. My aim was to practice for a couple of years and then train as a CBT therapist. I’ve most definitely been put off 😫😫
LikeLike
I was trained to deliver CBT when I was a social work practitioner. It was expected that we used it and assumed it was effective and appropriate for working with vulnerable young people with a myriad of socioeconomic and personal problems.
It wasn’t. I ended up co-working with 2 psychologists from CAMHS, delivering group work founded on a multi-theoretical and far more flexible, needs led and adaptive approach, which was MUCH more effective and appropriate.
Regardless of your view of CBT, the policy framework and the state application of CBT on an individual level to address politically constructed socioeconomic problems is of major concern at an ethical level. In this context it simply personalises the failings of neoliberalism, those failings do not reside “within” individuals – those are people failed by a system that cannot possibly address socioeconomic disadvantage, growing poverty and inequality. It is a system that perpetuates those things and adds to human misery.
LikeLiked by 2 people
I understand. So what you’re saying is that CBT is not the right method of therapy in this context. Are you still working as a CBT therapist? And also did you not gain any sense of fulfilment whilst in the job? Sorry for the bombarding of questions 🙈 but I don’t think I want to practice social work long term, and I would like to dive into the more therapeutic field
LikeLike
Yes, CBT is very limited and limiting in my opinion, in any context, but in the current one it is toxic and ideologically tainted, as it is simply being used to maintain the status quo and prop up a very damaging ideology of competitive individualism and economic productivity.
I wrote this longer piece a couple of years ago about CBT – https://kittysjones.wordpress.com/2015/03/22/the-power-of-positive-thinking-is-really-political-gaslighting/
I did get a lot of satifaction from my work, on a personal level. I also continued to do one to one work, as well as the group work. I couldn’t use CBT as it was mostly inappropriate for the circumstances of my clients. But social work under any tory government is stripped back. It’s been opened up to private services providers and will eventually be completely privatised. That’s big companies driven by a profit incentive, “efficiency” and savings, and a government agenda and contract, not thee delivery of real social work.
Social work long term = burn out. It’s underfunded, challenging, under-resourced and ultimately exhausting. I became too ill to continue in my role. The stress exacerbated my illness, I have lupus. You can’t liase with colleagues effectively, as they are all in the same situation.
The most rewarding therapeutic work I did was as a community based worker. That was about a lot of multipartnership working and much more ethically sound for me. I loved it. Again, under Conservative governments, youth and community work tends to be rolled back to bare bones, but the work and ethos is much more rewarding.
Hope that helps 🙂
LikeLiked by 1 person
I’m about to leave iapt after 8 years as a clinical lead in an iapt service. I think iapt is bad for the MH of staff, it’s become a battery hen farm for therapy and is at the mercy of endless random targets aimed at giving the conservatives sound bites to present to try an win votes but mean little. It’s all about massaging targets. Staff are trained to work in a highly protocolised system rather than think for themselves. I’m a clinical psychologist and don’t feel I can use my breadth of skill in this service so am leaving to work elsewhere. Iapt is highly politicised and that’s the problem.
But I do defend cbt, it can work wonders – I trained in it post doc long before iapt and use it flexibly along with other models, and for PTSD, OCD etc it can transform lives. It’s the system and the way iapt staff are trained as cbt technicians rather than therapists that’s to blame. Not cbt as a therapy.
I sure will be glad to leave though, I feel I’ve been pushed to burnout whilst trying to protect staff from the pressures and can’t do it anymore
LikeLike
I’m sorry to hear that, Emma. It’s the system, as you say. CBT has become a technocratic fix, rather than a therapy. And it’s crucial to have the freedom to use CBT with other therapeutic models as appropriate, too.
As you point out, CBT has become a poltical tool, to fit in with their “behaviour change” agenda. Because that agenda is founded on traditional Tory prejudices and a neoliberal view of relationships, it’s damaging all round. It’s become an adapted state therapy.
Best wishes.
LikeLike
Thanks Kitty for a really interesting piece – IAPT was essentially set up to get people off benefits and into a job. As you point out there is an assumption that work is good for mental health – yet these findings are on the back of department of health funded studies.
Work and jobs are two different things – if you are doing some sort of creative engaging work then of course it can be good but a job is a totally different thing – for most a job is made up of less than wonderful things like neat constant stress, boredom, meaninglessness, chronic routine, bullying, targets and is harmful to body, mind, spirit robs you of your precious time and energy diminishes our ability to care for self, others and develop meaningful community life – of course things need to get done but there are billions of us so surely its way over time for a proper debate on drastically reducing the working week, as proposed here http://neweconomics.org/2010/02/21-hours/.
IAPT workers are under increasing pressure and stress to simply service targets and process people as numbers – all anyone has time and energy to care about is two outcomes access and recovery – recovery in this context is meaningless, how can you recover from a toxic culture? well IAPT has the answer simply score below ‘clinical’ on two self assessment tick lists the PHQ9 and GAD7 and we have a winner – never mind the fact that these were developed be Pfizer, that all they captures is someones best guess at how they may or may not be feeling in a given subjective moment of time (with all the issues of introspection) with the powerful ‘expert’ sitting opposite you with all expectations that the scores will reduce – yet these scores are like god almighty within the service because they are linked to the micro management everyone is subjected to and the actual continued funding of the service, nuts right? the IAPT computer interface only promotes the medical model so everyone is assigned a label ‘depressed, anxious, ADHD, BI Polar, Personality Disorder etc there was once a category for stress but this has been removed. In order to meet targets staff are pressured to push people onto ‘courses’ and ‘online’ therapy because we’re told they have just as good evidence and outcomes – so that will be none then because there are all sorts of issues with the RCT model for testing a talking therapy. This book does a great job at covering the issues https://www.amazon.co.uk/Therapy-Industry-Irresistible-Talking-Doesnt/dp/0745329861
I also agree with your point about social worker = burnout – its a disgrace that this is just accepted for people that usually go into such work because they care and want to be helpful – burnout is a horrendous experience tantamount to abuse.
you might also find this article interesting regarding notions of recovery currently employed in the system https://brock.scholarsportal.info/journals/SSJ/article/view/1066/1036 and this mans work is really interesting http://www.davidsmail.info/introfra.htm and another interesting book on psychology and the system https://www.amazon.co.uk/Psychology-Capitalism-Manipulation-Ron-Roberts/dp/1782796541/ref=sr_1_1?s=books&ie=UTF8&qid=1504597823&sr=1-1&keywords=ron+roberts
be well
C
LikeLiked by 1 person
Thank you for an excellent, thoughtful and informative response, Chris. Will read the links
LikeLike
In Feb this year 2018 after waiting 9 months for an assessment counselling appointment my local MIND contacted me to tell me they ‘No longer offer counselling or benefit support services’ They now only offer IAPT and CBT – I contacted MIND who said ‘It’s up to individual branches’ – I did attend an IAPT course and was very lucky to have someone who was willing to support me as a person and mentioned nothing about my attitude etc. Once the sessions ended he was unable to refer me to anything other than MIND or the Samaritans
LikeLike
I don’t think CBT is bad per se, but has become reduced to a manualised treatment with politicised goals, those trained are less often psychologists with a broad empirical training than ‘technicians’. Used well and with good training CBT can be really effective. But it is not a panacea. Many iapt services only offer brief cbt and privately run services certainly are worse I think. but certainly the service I led offered counselling mindfulness CBT, EMDR and other interventions. Services are pretty much forced into following an identikit model and targets that are unrealistic and punitive (similar to education) – I found that following clinical integrity first off and trying to truly meet the needs of service users actually led to better target achievement. Those services who simply chase targets inevitably fail in the end. I agree that it’s now expected that iapt can do everything with money being cut in specialist services. There simply isn’t enough investment and not enough freedom to develop services creatively. I always said no to co-location in job centres because so much client distress was related to government policy and treatment by the state, poverty etc. Before iapt we had no services in most areas so the advent of therapy services was welcome. We need to take back these services and prevent them being political footballs and ensure we have a diverse range of therapies on offer. We must also not make blanket statements that cbt is bad or that all iapt services are bad – there are some good therapists albeit working in a very imperfect system.
LikeLiked by 1 person
Criticism is permitted, however. My main objection is that this therapeutic model is being used to prop up political ideology. But as someone who worked with the CBT model in a social services context, before we had the government we have now, I found it was problematic for other reasons too. I worked with 2 psychologists from CAMHS to develop a different model for family work,because of the shortcomings we experienced with CBT. Now, there doesn’t seem much scope to do that.
LikeLike
George Orwell’s ‘1984’ springs to mind here
LikeLiked by 1 person
Spot on
LikeLike
Just Wow!
A NICE game of Minecraft: philosophical flaws underpinning UK depression guideline nosology
Susan McPherson https://mh.bmj.com/content/early/2019/06/30/medhum-2019-011658
LikeLike