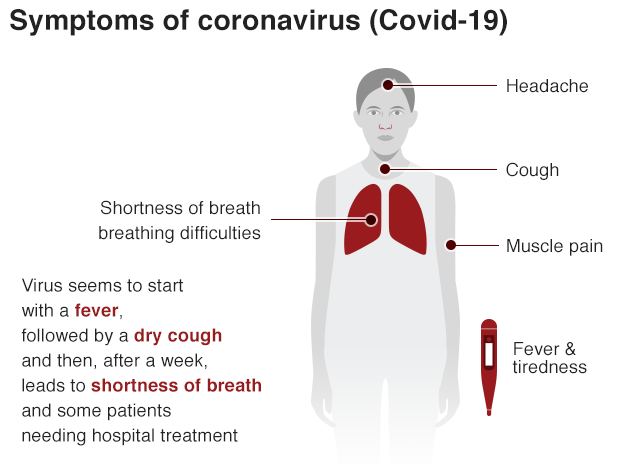
I can’t manage without my medication for systemic lupus erythematosus (otherwise known as SLE or lupus). Not being able to access my essential treatment places me at a significantly high risk of serious infections more generally, and specifically to covid-19 or a relapse, with severe complications such as severe pneumonia and sepsis.
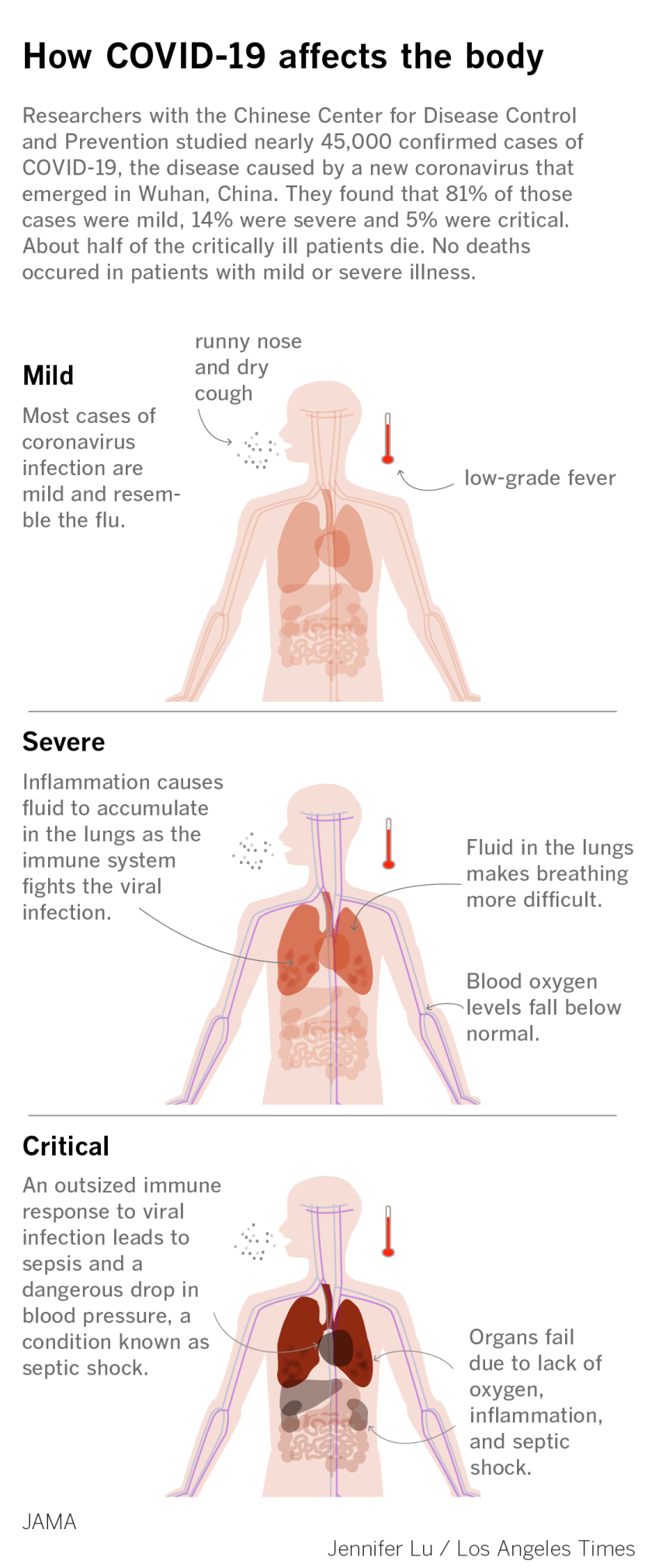
I was prescribed hydroxychloroquine in 2017 by my rheumatologist following life-threatening complications when I caught ‘flu. It happened during a flare-up of my autoimmune illness symptoms. Because lupus often lowers people’s immunity to pathogens, it leaves us vulnerable to severe infections and an abnormally aggressive immune response that causes inflammation throughout the body, and damages organs – sepsis. Within a couple of days of starting with ‘flu symptoms, I had advanced pneumonia and arrived at A&E already in septic shock. I very nearly died.
Many of the treatments used to treat severe lupus are immune suppressants. These also lower peoples’ resistance to infections, as do steroids, also commonly used to treat the widespread inflammation that autoimmune illness causes. I was originally prescribed injections of a chemotherapy called methotrextate to halt the advance of my illness.
I also periodically need slow release steroid injections to manage severe symptoms. Hydroxychloroquine is an anti-rheumatic, anti-inflammatory and antimicrobial drug that was originally used to prevent malaria. Studies show that it offers some protection for lupus patients with high risk of mortality from severe infections, such as pneumonia, kidney infections and sepsis.
It is the only medication shown to increase survival in lupus patients. It has been shown to reduce lupus flares and prevent organ damage including cardiovascular events, according to Andrea Fava and Michelle Petri in the Journal of Autoimmunity.
More recently, hydroxychloroquine has been researched for use in treating dengue, zika virus and HIV. It is a powerful antiviral.
That is why it has gained attention from governments around the world as a potential treatment for covid-19.
Recently, the UK government has banned the parallel export and “hoarding” of three drugs being used to treat coronavirus patients in China in anticipation of shortages in Britain following the covid-19 pandemic.
Parallel exporting is when wholesalers buy medicines already placed on the market in the UK to sell them in another country in the European Economic Area (EEA). Parallel exporting and hoarding of medicines by wholesale dealers can create or worsen medicine shortages.
Chloroquine phosphate and the generic drug hydroxychloroquine (both anti-malarials) as well as a couple of other antivirals, are being restricted to “meet the needs of UK patients”, the government has said.
However, it wasn’t specified which patients’ needs are to be met. It’s emerged since that the government clearly didn’t mean lupus patients like me who depend on the drug to prevent our illness from becoming life-threatening.
While the infection rate and severity of covid-19 remain moving targets for much of the general public, people who suffer from lupus are immunocompromised, placing us at significantly higher risk of becoming seriously ill. In addition, many people with lupus have a complement deficiency, which makes us even more vulnerable to serious infections. The blood complement system involves both the innate and the adaptive immune systems. Systemic lupus erythematosus is associated in particular with low C3 and C4.
Hydroxychloroquine was placed on the restricted list from 14 March and chloroquine phosphate – an older anti-malarial, was added on 26 February.
Following Donald Trump’s personal take on public pharmaceutical advice regarding the treatment of covid-19 with chloroquine, a man in Arizona died after ingesting chloroquine phosphate – believing it would protect him from contracting coronavirus. His wife also ingested the chemical and is receiving critical care. She said they had watched the US President speaking about the potential (but unverified) benefits of chloroquine treating coronavirus during televised briefings.
However, the toxic ingredient the couple in their sixties consumed was not the medication form of chloroquine used to treat malaria and autoimmune illness in humans, but the ingredient listed on a fish tank cleaning agent, which is used to treat parasites in fish.
As someone who takes hydroxychloroquine every day, and who was clinically assessed as having covid-19 two weeks ago, when the symptoms I’d already had a month by then took a turn for the worst, I can say with confidence that the drug does not prevent infection with the coronavirus. I can say, however, that perhaps my daily dose is a reason why I didn’t end up needing intensive care support. That said, I’m still treading water with symptoms six weeks from the onset, though at least the awful chest pain has receded.
The UK government says: “Chloroquine and hydroxychloroquine are not licensed to treat covid-19 related symptoms or prevent infection.
“Clinical trials are ongoing to test chloroquine and hydroxychloroquine as an agent in the treatment of covid-19 or to prevent covid-19 infection. These clinical trials are still not completed, so no conclusions have been reached on the safety and effectiveness of this medicine to treat or prevent covid-19.
Until we have clear, definitive evidence that these treatments are safe and effective for the treatment of covid-19, they should only be used for this purpose within a clinical trial.”
Yet pharmacies are now reporting shortages of hydroxychloroquine.
Hydroxychloroquine is a front line medication taken by approximately 90% of lupus patients to control their condition.
LUPUS UK, a national charity, have been receiving an increasing number of reports from people with lupus who have been unable to collect their prescription, with their pharmacist currently unable to order the medication from their suppliers.
The charity says: “We don’t yet know how effective hydroxychloroquine might be against covid-19. What we do know, is that if people with lupus who have been prescribed hydroxychloroquine stop taking this medication, their disease could flare.
“This can in itself be a life-threatening situation, unnecessarily burdening the health service, but it also increases the vulnerability of already at-risk patients to covid-19 infection.
“Given this, we have acted early and written to the Secretary of State for Health and Social Care (Matt Hancock) and the Chief Pharmaceutical Officer with other member of RAIRDA, asking them to ensure that the supply of hydroxychloroquine to patients remains secure and to look into how we can make this supply even more robust in the coming months.
“On the 24th March 2020 Daniel Zeichner MP submitted a written question to the Department of Health & Social Care;
“To ask the Secretary of State for Health and Social Care, what steps he is taking to ensure a robust supply of hydroxychloroquine to patients reliant on that medication to manage (a) lupus, (b) scleroderma, (c) rheumatoid arthritis and (d) other serious autoimmune rheumatic conditions during the covid-19 pandemic.”
We are awaiting a response.”
Lupus UK add: “We know that lots of people have had issues collecting their prescription of hydroxychloroquine and want to help us.
Writing to or emailing your local elected representative such as your Member of Parliament (or other local representative such as your Welsh Assembly Member, Member of the Scottish Parliament or Members of the Legislative Assembly in Northern Ireland), can be a way of expressing your concerns and supporting RAIRDA’s work asking the government to take early action to prevent any prolonged shortage.
This will not only help patients, but also help reduce demand on the health service at this difficult time.
It’s important your letter or email is your own and says why this issue is important to you as a individual, but here are some things you might want to consider:
- Checking who your MP is HERE. Include your name and address at the beginning or end of your email – politicians can only respond to people who live in their constituency, so make sure you write to the correct MP and show them you’re a constituent.
- Using a mix of your own personal story and concerns and facts about the wider context, like the fact a shortage of hydroxychloroquine could mean patients flare and need to go to hospital, putting more burden on the health service at this really difficult time.
- At the end of your letter, perhaps ask them to raise this issue with the government urgently.
- You might want to include some general information about hydroxychloroquine, like this below:
Hydroxychloroquine is used to control some rare autoimmune rheumatic diseases like lupus and scleroderma. These can be life-threatening if they aren’t controlled. Tens of thousands of people in the UK therefore rely on this medication. Without this medication patients conditions can flare, which can be really serious, life-threatening, and it can also make people with these conditions even more vulnerable to covid-19.
Shortages of the drug have been reported because it’s being considered as a treatment for covid-19. However, it’s still unproven. While we don’t know much about hydroxychloroquine’s ability to treat covid-19, we do know that it helps patients with conditions like lupus and scleroderma control their diseases, helping them stay relatively well and reducing the burden on the health service.”
If you’re writing to a member of a devolved assembly follow these links to find your local representatives in:
If you have experienced difficulty getting your hydroxychloroquine prescription, please contact Lupus UK here.
More information will be shared as the situation develops.

If you don’t need it, please leave it for those whose lives depend on it.
—
See also: Vital drug for people with lupus running out after unproven Covid-19 link
It is easier than ever before for those with vested interests to spread disinformation on vital matters of public interest. It’s happening every day.
If you want to know what’s really going on, you need to hear from the those willing to dig down to the truth. But I can’t do that vital work unless readers donate.
Please consider making a donation. That ensures I can continue to research, write independent articles and support others facing the injustices of Conservative anti-welfare policies.
At the moment I am struggling to get by in quarantine. I rely on online shopping at the moment, but most supermarkets are fully booked up, even for ‘click and collect’ slots. That leaves me with the only desperate option of buying food and essentials on ebay and other sites where prices have been spectacularly hiked.