Yesterday on Twitter, I posted one of my previous posts – Jobcentre tells GP to stop issuing sick notes to patient assessed as ‘fit for work’ and he died – in which I discuss a letter addressed to a GP regarding a seriously ill patient. It said:
“We have decided your patient is capable of work from and including January 10, 2016.
“This means you do not have to give your patient more medical certificates for employment and support allowance purposes unless they appeal against this decision.”
The patient, James Harrison, had been declared “fit for work” and the letter stated that he should not get further medical certificates.
However, 10 months after the Department for Work and Pensions (DWP) contacted his doctor without telling him, he died, aged 55. James clearly wasn’t fit for work.
The GP had stopped issuing medical certificates when the DWP told him to. It is completely unacceptable that James Harrison was left struggling without support, when he was clearly very ill. It is also unacceptable that James’ GP was given instructions from the state – that caused harm – without James’ knowledge.
The certificates – so-called fit notes – demonstrate that the government seems to have some difficulty in recognising that sometimes people get ‘sick’ and require support via the provision they have paid into.
Austerity: When the state takes money from the public and hands it out to millionaires
David Cameron, however, had other plans for the UK. He said: “We simply have to get to grips with the sicknote culture that means a short spell of sickness absence can far too easily become a gradual slide to a life of long-term benefit dependency.
“The new welfare bill – described as the biggest shake-up of the system since it was set up 60 years ago – is designed to say end the culture of the fit and healthy being able to refuse work being rewarded for staying at home.”
However, the statement isn’t coherent. He infers that people are recovering from a brief period of illness and then refusing to return to work. As we have learned at great human cost over the last few years, this legislation has destroyed the lives of thousands of people who are ill. It was always intended to take away support from those who need it most. That is evident in the Conservatives’ incoherent attempt at a justification narrative, propped up by the right wing media.
It never seemed to have crossed Cameron’s mind that 1) people’s medical conditions may worsen, they may have a chronic or degenerative illness. Being chronically ill does not make a person ‘benefit dependent’, it simply makes them ill. 2) The public contributes to the treasury, which is in part a funding mechanism towards social security and other state provisions, via tax and national insurance. This is done on the understanding that the state ensures that citizens can meet their basic survival needs. The Conservatives have clearly stated they have ‘other’ ideas on how our public funds should be spent, which does not include meeting the needs of the public.
The state is responsible for handling public funds. It is unacceptable that such contentious neoliberal ideology is being used by the Conservatives to dismantle state provision for those who need it most, while deliberately targeting the poorest citizens with austerity cuts. Meanwhile, millionaires are rewarded with generous tax cuts from the public purse. At the time when the welfare reform act was passed, millonaires were handed a tax cut of £107,000 each per year. This callous and unjustified approach to social administration is destroying people’s lives and has profoundly damaged our democracy and society, while seriously and systematically violating the human rights of the UK’s most marginalised groups.
It is very worrying that the clearly dangerous ESA65B form is a standardised response to GPs from the DWP following an assessment where someone has been found fit for work. I discussed some of the raised issues further in another article from last year that I posted on Twitter yesterday – GPs told to consider making fit notes conditional on patients having appointment with work coach.
It’s even more worrying that the part clarifying ‘fit notes’ should continue if a person is appealing a ‘fit for work’ has been removed from the standard letter, and a line added that says: “In the course of any further consultations with […] we hope you will also encourage [the patient]in [their]efforts to return to, or start, work.”
I always worry when the government uses the words “encourage”, “help” and “support” in the context of policies and political practices that affect disabled people. They are usually techniques of neutralisation – euphemisms for the actions embedded in punitive and harmful policies.
This growing practice of the state intruding in the confidential relationship between a GP and patient undermines trust, it damages the professionalism and clinical expertise of doctors and threatens the safety and wellbeing of patients. It shrinks the safe spaces for citizens to escape the increasingly oppressive practices of the government. It turns GPs into non-neutral agents of the state.
We know from the high rate of success at appeal for Employment and Support Allowance claims that the DWP’s decision making regarding ill and disabled people’s ‘work capability’ is truly atrocious and negligent, and there is absolutely no convincing empirical evidence that “work is a health outcome”. (See: Work as a health outcome, making work pay and other Conservative myths and magical thinking.)
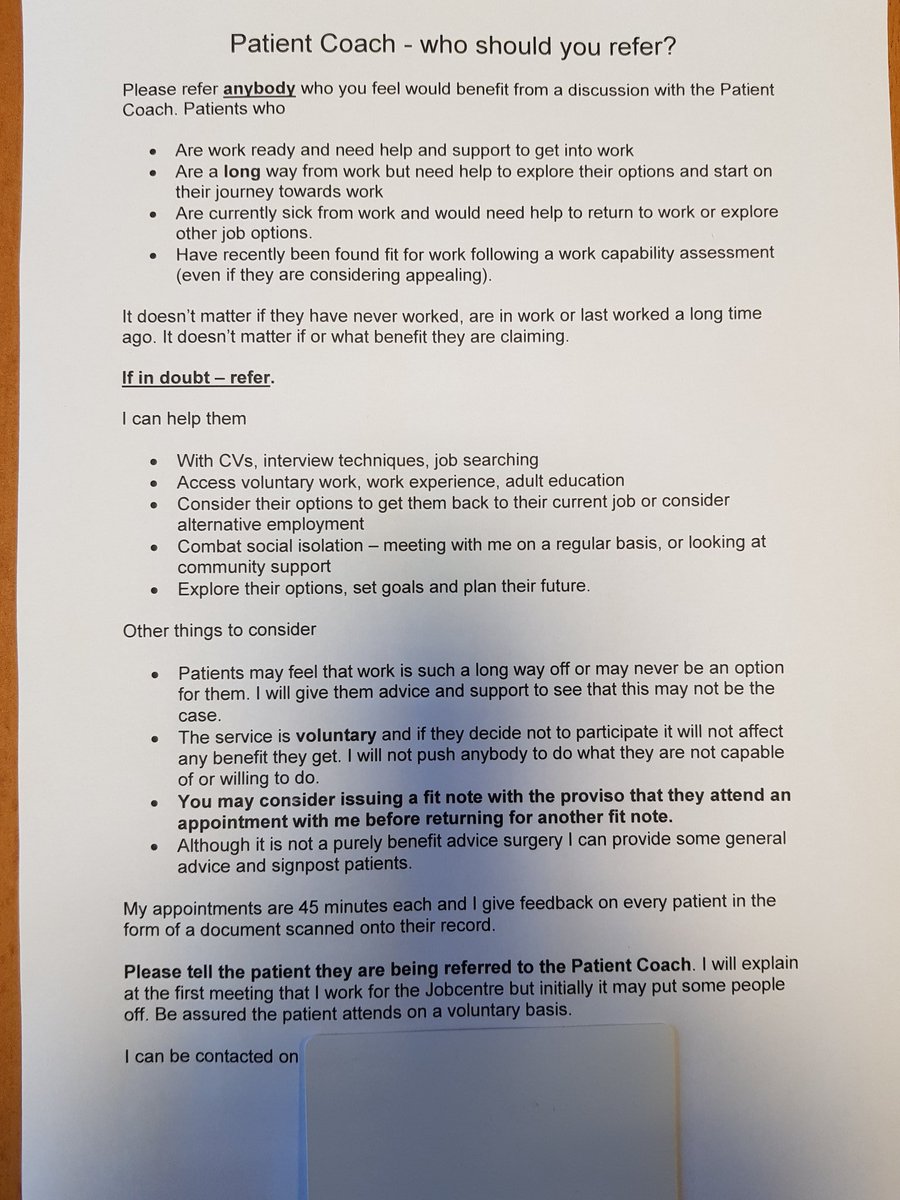
Last year, jobcentre staff were forced to withdraw guidance that urged GPs in Leeds to use deceitful tactics to attempt to get people who are ill off social security support and into work. The shocking guidance asked doctors to send patients for a 45-minute session with a “Patient Coach” – without mentioning that the coach actually worked for the the DWP.
It was even suggested that GPs withhold sick notes unless patients agreed to attend an appointment with the work coach.
This is a tactic many of us have previously warned of – the government attempting to co-opt doctors to police ill and disabled people, pushing them into work, regardless of whether or not it is appropriate or safe to do so. But it also indicates the direction of travel for healthcare in the UK. The government intend to make that provision conditional also. (See Tories propose nudge, big business AI initiative and ‘personal responsibility’ in place of adequate health care funding.)
The government is forcing people who are ill into either work or into poverty, and both outcomes are absolutely ethically unacceptable, a violation of rights, authoritarian and very dangerous. Increasingly, poverty is being used as a weapon to coerce people into work. However, many jobs are not paying enough for people to meet their living costs, so it is no guarantee that work will alleviate poverty.
The government seems to think that citizenship rights ought to be entirely conditional on people being economically useful to the government.
If we fail to be so, we are being treated as disposable political commodities. But citizens are not a means to state imposed ends and ideological aims in wealthy so-called first world democracies. And democratic governments don’t generally impose ‘behavioural change’ techniques on citizens, or professionals, for that matter, in order to make them complicit in the abuse and oppression of marginalised groups. The state is increasingly policing and punishing the poorest citizens, leaving them completely isolated and without any reliable support whatsoever.
The ESA65B is misleading GPs and deterring people from appealing wrongful DWP decisions
On the DWP’s ESA65B GP’s letter template most recently placed on the government site, titled “Help us support your patient to return to or start work” it says: “We assessed [Title] [First name] [Surname] on and decided that [select] is capable of doing some work, but this might not be the same type of work [select] may have done before.
“We know most people are better off in work, so we are encouraging [Title] [First name] [Surname] to find out what type of work [select] may be able to do with [select] health condition or disability through focused support at [select] local Jobcentre Plus.
“In the course of any further consultations with [Title] [First name] [Surname] we hope you will also encourage [select] in [select] efforts to return to, or start, work
“Please do not give [Title] [First name] [Surname] any more fit notes relating to [select] disability/health condition for ESA purposes.
The problem is that people appealing wrongful DWP work capability decisions need to provide sickness certification in order to proceed.
Minister for disabled people, Sarah Newton, responded to one of several Written Questions from Emma Dent Coad, saying: “The ESA65B letter is issued to GPs in every case where an ESA claimant has been found ‘fit for work’. This process was built into the IT system as part of the introduction of ESA in October 2008.
“Following a Ministerial requirement by the Cabinet Secretary, which was endorsed by the Secretary of State for Work and Pensions, the content of the ESA65B letter has been improved in order to explain to GPs the type of support customers can expect to receive from their local Jobcentre, and to ask GPs to encourage customers in their efforts to return to work.” [My emphasis].
GPs are trained and tasked to objectively address health and wellbeing, they should not be co-opted as government ideologues.
The decision to change the letter template was made without any scrutiny from or consultation with parliament and the public. It’s worth reading the series of questions by Emma Dent Coad. Prompting accountable and transparent answers from Sarah Newton appears similar to an exercise in pulling teeth. The responses given display the arrogance, contempt and delusions of an authoritarian government.
When people become ill, they make an appointment with my GP, and not the secretary of state for work and pensions, and for very good reasons. People need support and treatment, not someone spouting ideologically orchestrated dangerous claptrap about how work is ‘good’ for them. It seems the notion of convalescence and recovery are incompatible with the government’s aim of “getting Britain working”.
Catastrophically inaccurate assessments within the DWP are the norm. The government are intentionally reducing access to essential support and services for ill and disabled people, and this ideological attack is causing material hardship, suffering, distress and sometimes, it is killing people.
The contentious “fit for work” assessment is forcing severely ill people to look for work and sanctioning them if they’re exhausted, in too much pain to get out of bed, while delays in social security are forcing cancer patients to food banks, and the bedroom tax results in bed-bound ill and disabled people facing horrifying threats of eviction.
These are the direct consequence of intentionally punitive government policies, which aim at enforcing ‘personal responsibility’ and ‘behavioural change’ on those citizens with the fewest choices.
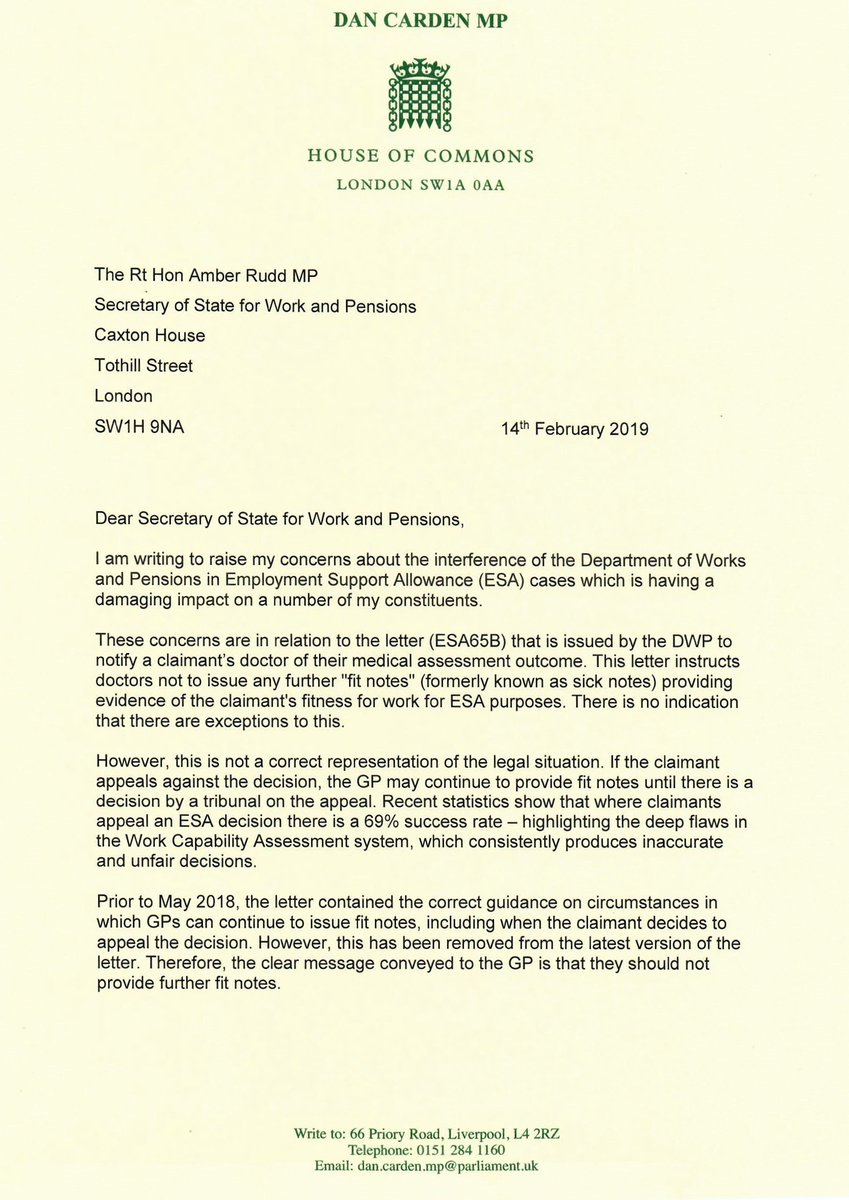
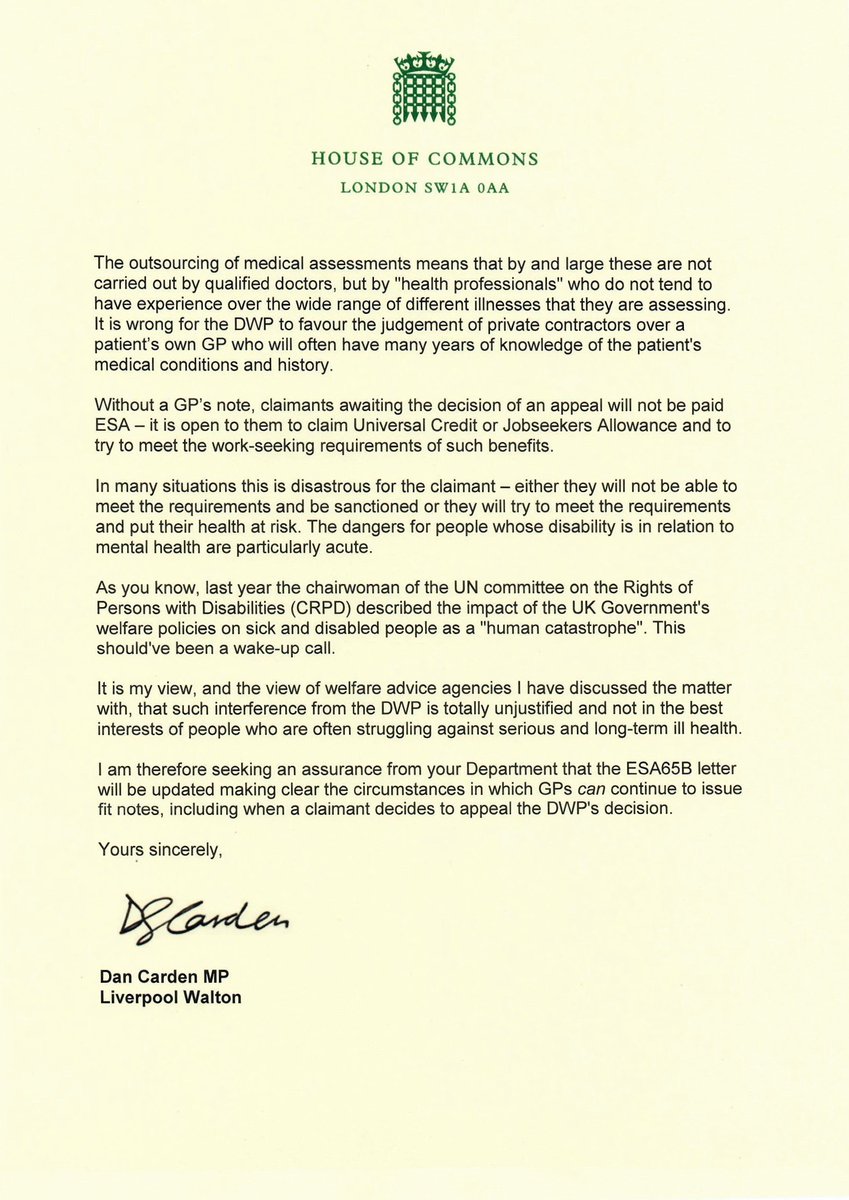
Dan Carden’s letter to Amber Rudd
I was pleased to see Liverpool Walton MP Dan Carden’s letter to Amber Rudd (below) which addresses some of the concerns many of us have raised. He also notes that without a GP’s ‘fit note’, (the Conservative’s Orwellian rebrand of the sick note) it isn’t possible for people challenging Department for Work and Pensions (DWP) decisions to claim Employment and Support Allowance (ESA) in the interim period, until their appeal is heard at Tribunal.
Indeed, people who have lodged an appeal against a wrongful decision have been blocked from claiming ESA while awaiting the hearing, due to the misleading letter routinely sent from the DWP to doctors. This prevents untold numbers of low-income claimants from accessing financial support while they wait for months on end to go to tribunal.
Entitlement to ESA pending appeal is enshrined in the ESA Regulations to cover the whole of the period leading up the hearing. It is also possible to have the payment backdated to cover the Mandatory Review waiting period too – it can take over six weeks for the DWP to review their original decision, over which time people are left without welfare support.
However, ESA pending appeal is not paid automatically – people usually have to ask for it, and must provide fit notes from their GP, presenting these along with their appeal acknowledgment letter from the Tribunal Courts to their local Job Centre. The Job Centre should report back to the DWP who will arrange for ESA pending appeal to be paid.
It simply isn’t appropriate for the DWP to interfere in a GP’s professional and qualified judgement, especially given the high rate of successful ESA appeals, indicating just how poor the decisions issued by the DWP actually are concerning people’s capacity to work.
Dan’s letter:
Related
Jobcentre tells GP to stop issuing sick notes to patient assessed as ‘fit for work’ and he died.
GPs told to consider making fit notes conditional on patients having appointment with work coach
Rogue company Unum’s profiteering hand in the government’s work, health and disability green paper
I don’t make any money from my work. But you can contribute by making a donation and help me continue to research and write informative, insightful and independent articles, and to provide support to others. The smallest amount is much appreciated – thank you.